
Explosive Corona Papers: Tens of Thousands of Additional Deaths in Austria
An internal study prepared for the government by a commission of experts on the COVID19 crisis shows a gloomy forecast for Austria. The paper states that under the realistic assumption of a replication factor of 1.7 (i.e. 1 person infects 1.7 people), the Austrian health system will collapse. If it is not possible to push the replication factor below the value of 1, tens of thousands of additional deaths and a collapse of the health care system can be expected in Austria by mid-April.
 Austria's primary goal must be to push R0 below 1. This will probably require much stricter measures than those currently in force. Under the realistic assumption of R 0 = 1.7, the Austrian health system will collapse in mid-April. / Picture: © Vindobona.org (Collage of Photos)
Austria's primary goal must be to push R0 below 1. This will probably require much stricter measures than those currently in force. Under the realistic assumption of R 0 = 1.7, the Austrian health system will collapse in mid-April. / Picture: © Vindobona.org (Collage of Photos)
The statement of an expert advisory board of the government on the COVID19 crisis reveals explosive figures.
For an epidemic, the decisive factor is the replication factor R 0.
This is the average number of people that an infected person in turn re-infects.
If this number is less than one, the epidemic decays with exponential speed.
If it is greater than one, the epidemic inevitably spreads at an exponential rate.
If it is not possible to quickly bring the factor R 0 below the value of 1, tens of thousands of additional deaths and a collapse of the health system are to be expected in Austria, according to the study.
In some Asian countries it has been possible to prevent the outbreak of the epidemic completely (Taiwan, Singapore) or to contain an epidemic that initially spread unchecked (China, South Korea). These countries have managed to reduce the replication factor R 0 from initial values of about 4 to a value below 1.
This was achieved by means of country-specific packages of measures without causing lasting damage to the economy.
In Europe, there is little solid empirical evidence for a significant decline of R 0.
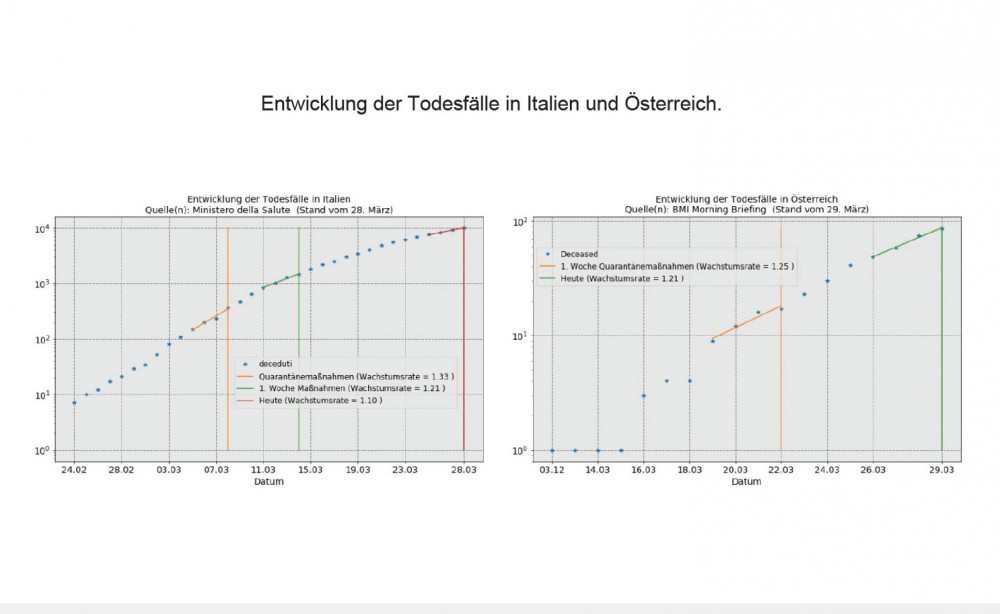
In fact, the registered COVID 19 deaths are the only reliable data available to date that allow conclusions to be drawn about the development of the factor R 0. Their course follows with a delay of about 14 days parallel to the course of the infections.
An empirical glimmer of hope in Europe comes from Italy.
Severe restrictions were imposed there on 8 March, one week earlier than in Austria. This meant that enough time had already passed for the effect of the restrictions to be reflected in the number of deaths. Fortunately, for some days now, the daily relative increase in deaths in Italy has been falling from 1.33 (three weeks ago) to 1.10 (average of the last 4 days).
This number must fall permanently below the value of 1.07 (which corresponds to a replication factor of R 0 = 1) in order to have a chance of containing the epidemic. In Italy, we are still a long way from achieving this, despite the very strict measures that have now been taken.
In Austria, since the introduction of sanctions, the daily relative increase in deaths has fallen from 1.25 to 1.21. However, these data are subject to great statistical uncertainty, as the number of deaths in Austria is fortunately still low. The data point in the right direction, but do not yet allow any valid statements to be made.
MATHEMATICAL MODELS
The internationally favoured epidemological forecast model (the authors' implementation is derived from the SEIR models from Basel and Harvard) is based on a list of specifications for relevant factors (such as factor R 0 ). From these assumptions the development of the relevant epidemic groups (infected, sick, intensive care patients, dead) follows in a logically compelling way.
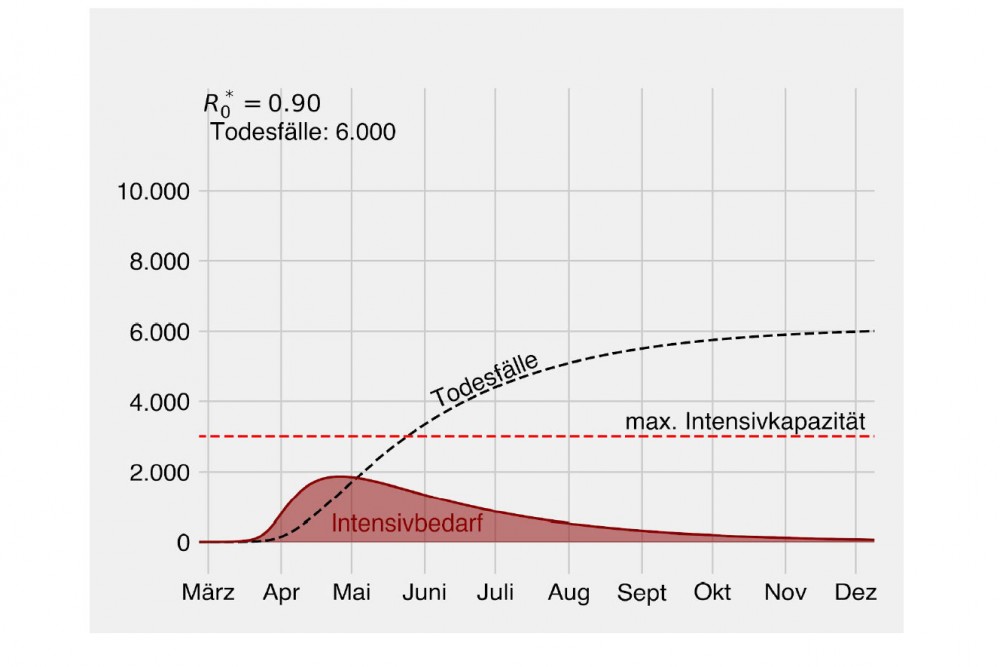
Like any mathematical model, it can only make statements of the form "if, then". The authors have adapted the SEIR model to the Austrian situation. If a value of R 0 = 0.9 is given, the following development results, for example, in the demand for intensive care beds and the expected number of deaths:
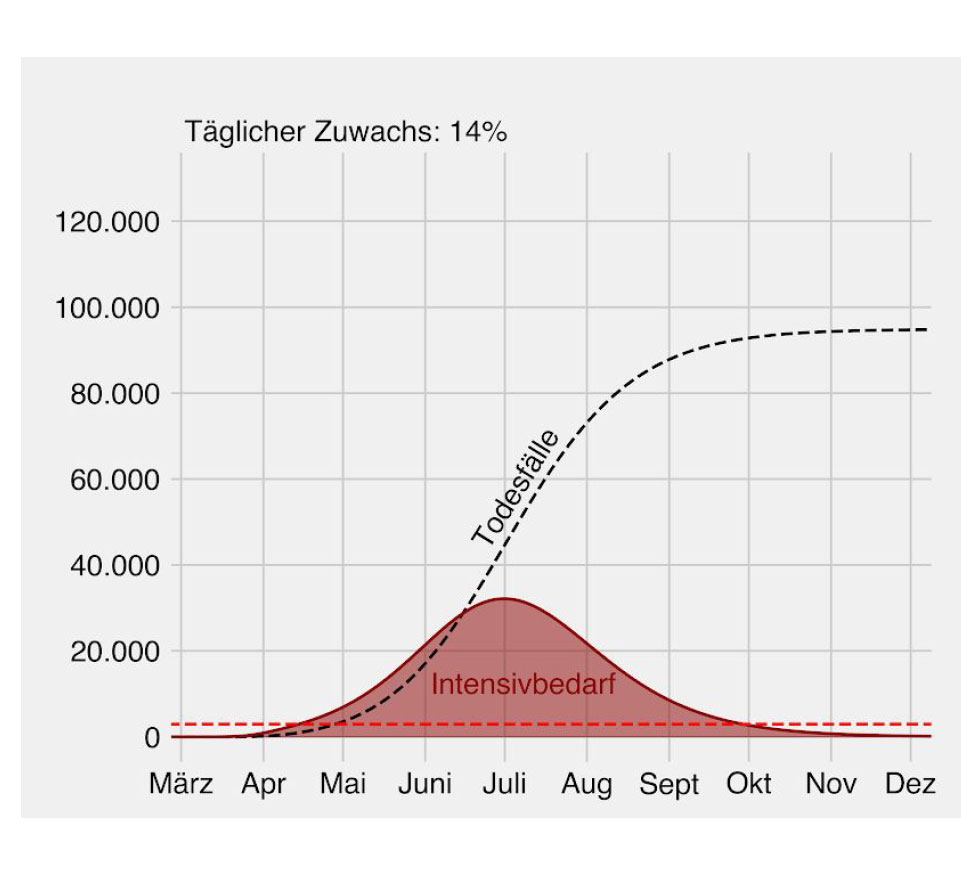
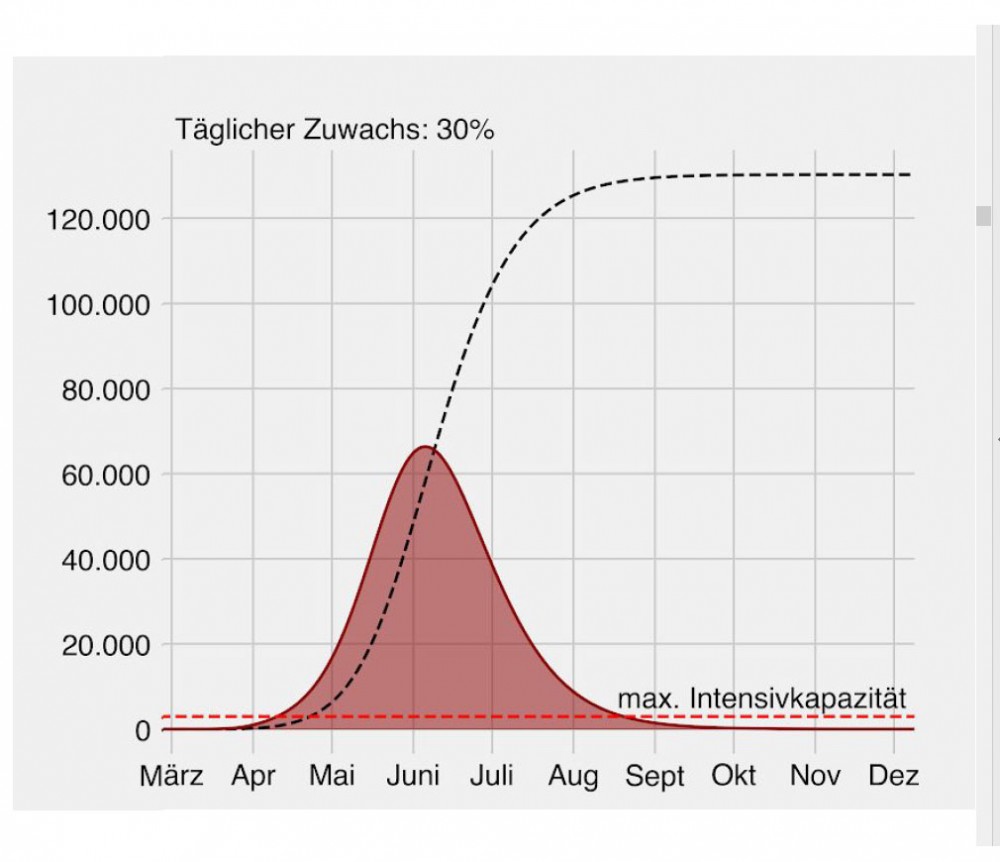
However, this development depends decisively on the optimistic assumption R 0 = 0.9. On the other hand, if the authors assume a daily increase in the number of infected persons of 14% (as currently estimated in Austria) or 30% (as at the beginning of the epidemic) for the future, the following development results:
The model is well suited to analyse changes in the underlying parameters.
The authors have extrapolated the development in Austria under the following two alternative assumptions:
A. Avoidance of any transmission by health personnel (which requires regular testing, protective clothing and strict isolation)
B. Healthcare workers as the main vectors "superspreaders", as observed in Italy (10% of all infected persons there are healthcare workers, > 50 doctors died)
There is a strong effect on the congestion in the intensive care sector and the expected death figures in Austria.
This is just one example of how this model can be used to analyse the change in specifications. For the evaluation of other planned measures, this tool - ceteris paribus - can provide analogous estimates of the consequences at the push of a button.
RECOMMENDATIONS
A. Central recommendation:
The primary goal must be to push R0 below 1.
On no account should hopes be raised for a speedy relaxation of the restrictions.
This will probably require much stricter measures than those currently in force.
Under the realistic assumption of R 0 = 1.7, the Austrian health system will collapse in mid-April. There is little time to prevent this.
The example of Wuhan also gives hope: after China managed - in two steps - to push the value of R 0 down to 0.32 there, the crisis was overcome within a few weeks.
The mix of restrictions can be changed.
For example, with compulsory masking in public places and greater use of testing.
Both measures were practised by all successful countries.
But the overall impact of the mix on the value of R 0 must not deteriorate under any circumstances.
Of course, all this only applies until the widespread use of vaccination is possible.
B. Specific suggestions for special measures:
1. rigorous implementation of the previous measures: e.g. control of the number of customers in the supermarket by security personnel, rigorous warnings in the event of non-compliance.
2. special focus on medical staff, especially through regular testing. This would certainly be positively received by this extremely exposed group of people.
3. measures to contain infection by asymptomatically infected persons, such as supermarket staff. Increased testing, including tests from research laboratories that have not yet been validated.
4. increased use of face masks (if supply is guaranteed). Although the individual protection of face masks may not be very high, the statistical effect on the spread of the disease seems to be considerable.
5. tracking of contacts of infected persons in the days before the test with the help of mobile phone data.
6. risk groups and especially those with mild symptoms should be better isolated. Ideally, a food supply service should be organized for the risk group.
7. establishment of special "fever hospitals", i.e. facilities specially reserved for Covid19 infected persons.
The study was prepared by the following authors with the support of the rectors Heinz Engl (Uni Wien) and Markus Müller (Med Uni): Mathias Beiglböck (Uni Wien), Philipp Grohs (Uni Wien), Joachim Hermisson (Uni Wien, Max Perutz Labs), Magnus Nordborg (ÖAW), Walter Schachermayer (Uni Wien).